Erythritol is a natural, sweet ingredient that is a useful tool in the healthy sweetness toolkit. Despite years of scientific studies and evidence for its safety and even potential health benefits, there is still widespread confusion about its origin, usage, metabolic pathway and biological relevance. With decades of scientific scrutiny, research and analysis to draw from, this is a very concise summary to clarify to the general public, what endogenous (body-produced) erythritol is, erythritol as an ingredient, and what ‘happens’ to it in the body. This is ALSO an analysis of the recent publication by Witkowski, M. et al. Keep reading if you care about what it all means for your health and food choices.
- A) Endogenous erythritol is produced from Glucose Metabolism in the Pentose Phosphate Pathway (PPP). What is one key function of the PPP? In addition to maintaining carbon homoeostasis, providing precursors for nucleotide and amino acid (protein) synthesis, providing reducing molecules for anabolism, a KEY FUNCTION is to counteract oxidative stress. In the context of high blood glucose (pre-diabetes, diabetes, metabolic dysfunction), there is higher PPP flux and higher levels of its metabolites, incl. erythritol. This endogenous erythritol is in fact a widely known biomarker for cardiometabolic dysfunction and thus it is NOT surprising if found in higher amounts in those with cardiometabolic dysfunction. Given evidence for erythritol as an antioxidant, if we were to blame this biomarker for the dysfunction which elevates it, could we in fact be blaming (correlation) the firemen for causing the fire — oxidative stress — that was originally caused by hyperglycaemia due to insulin resistance? What is a key cause of hyperglycaemia and insulin resistance? Excess SUGAR intake.
- B) Erythritol as ingredient: Erythritol is naturally occurring in various fresh fruit, vegetables, mushrooms, and fermented foods. As an ingredient it is produced by fermentation from food and thus is classified as natural and can be certified organic when meeting organic standards. It is 70–80% as sweet as sugar. Not many food/beverage products are sweetened with erythritol alone, as it has a cooling effect in the mouth if too much is used. Thus, it is normally combined with a higher-sweetness ingredient such as monk fruit extract or stevia extract. Thus, in any food/beverage package, the amount of erythritol will usually be max. 10-12g (in a 330ml can, max 11.55g). How much one absorbs also depends on if it is in food (with fiber and other components), or in liquid form (with water only). We must always consider what we ingest, what we actually absorb from what we ingest, what is the ‘fate’, signalling, and other effects of that food/drink inside the body.
Metabolic Pathway when Ingested: Multiple human trials demonstrate that erythritol is absorbed in the small intestine and c. 80% is excreted unchanged, via urine within 24hrs. This study tested a high amount: ingestion of 1g/kg body weight. The same study noted, “Less than 20% of erythritol remained unabsorbed and was available for colonic fermentation and potential production of short-chain fatty acids.” Subsequent research in the British Journal of Nutrition indicates that the unabsorbed amount is in fact not fermented and is also excreted unchanged, in feces. Another study found that with ingestion of 20g in liquid, 82% was excreted unchanged in urine within 24hrs. Yet another human study found that after ingestion of 0.3g/kg body weight, 86% was excreted unchanged in urine in 24hrs, and 90% by 48hrs. Thus, erythritol is not metabolised for energy, and 90–100% of it is EXCRETED UNCHANGED. Important to note is that whereas other polyols (e.g. maltitol, xylitol, sorbitol) in quantities found in food products can cause osmotic pressure, diarrhea and bloating, because of its low molecular weight, this is NOT the case for erythritol.
Research History & Safety: Erythritol has been used as a sweet ingredient in Japan since the 1990s. It was approved GRAS in the US in September, 2001. It was approved in the EU first in 2003 as an additive (small amounts), then as a sweet ingredient in 2006, then as an additive in drinks (small amounts) in 2010, and finally as a sweet ingredient in drinks in 2015. Approval was based on evidence from numerous short-term and long-term studies in humans and animals on its absorption, distribution, metabolism, excretion, and toxicity. Studies repeatedly demonstrated the same metabolic pathway as described above (excreted unchanged, on osmotic pressure), and even in very high doses over long periods, demonstrated that there was NO general toxicity, no kidney toxicity, no carcinogenic activity, and no developmental nor reproductive toxicity.
Erythritol Health Benefits:
- It may help with satiety (fullness) and suppress hunger (ghrelin), also shown here in another study.
- It has anti-inflammatory effects and may improve glucose tolerance.
- It may ameliorate several metabolic parameters including hepatic (liver) triglyceride and free fatty acid levels.
- It reduces pathogenic dental plaque.
- It has antioxidant impacts.
ANALYSIS of Witkowski, M. et al.: Do firemen cause fires?
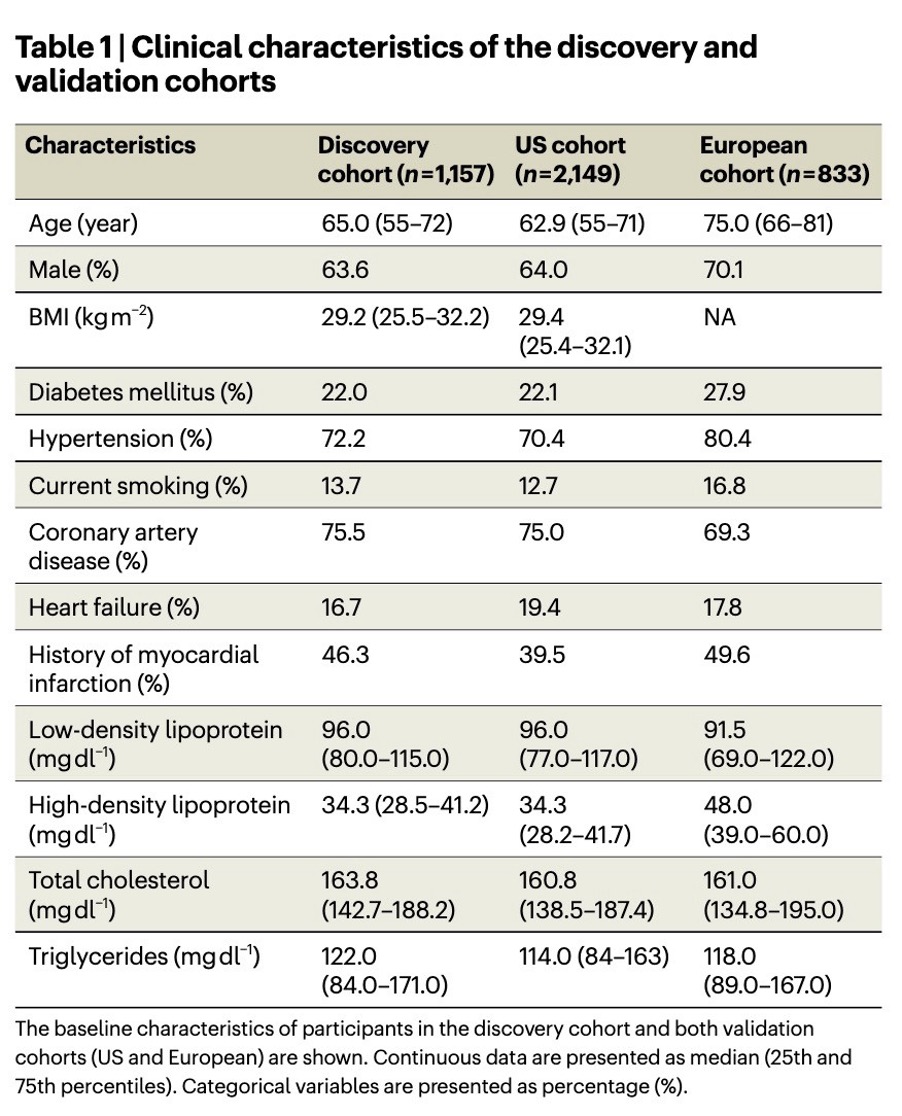
Part 1: This study looked at previously collected samples of patients who had “high prevalence of CVD and risk factor burden, including type 2 diabetes and obesity”. Below is a description of these very unwell patients. To highlight:
- 69–76% had Coronary Artery Disease
- 70%-80% had Hypertension
- 22%-28% had diagnosed Diabetes
- Average BMI was 29 (borderline between overweight | obesity) in the US cohorts
- 40–50% had a history of myocardial infarction (MI)
Problem 1: The study implies that INGESTED erythritol leads to higher levels of fasting erythritol and that this has some causal effect in leading to major adverse cardiovascular events. “In both validation cohorts, plasma levels of erythritol were higher among individuals with prevalent CVD; higher levels of erythritol were also observed among those who experienced an incident MACE over the ensuing 3 years of follow-up.” The US data was collected in 2001. Erythritol was only approved in September 2001. As for the European data, it also was collected just after the EFSA approved erythritol for use in beverages (which by the way is limited to 1.6% by volume, i.e. 5.3g in a 330ml drink). They say it was collected “well into 2018”. However, compared to the US, consumption of sugar-free products in Europe was/is less. Furthermore, as 2 of the 3 cohorts were from the US, the erythritol measured in the plasma was ENDOGENOUS erythritol.
This is a MAJOR problem because so much of the paper implies that ingested — not endogenous — erythritol is causing an issue. They even contradict themselves within the paper on this point: “obesity (that is, individuals for whom avoidance of sweets and weight reduction efforts are routinely recommended)” — implying that these people were being recommended to eat the erythritol-sweetened sugar-free products that were NOT EVEN AVAILABLE on the market yet. Then in the discussion they admit that the erythritol measured was endogenous: “While fasting samples in the US validation cohort (where enrollment largely preceded proliferation of erythritol in processed foods) likely reflect endogenous levels”.
Problem 2: HELLO REVERSE CAUSALITY.
For reasons unknown, the authors acknowledge that “Erythritol is endogenously produced by the pentose phosphate pathway and the metabolite is readily observed in the circulation”, yet they do not mention that it is widely known in the scientific literature as a biomarker of upregulated PPP, which itself is a sign of cardiometabolic dysfunction. Upregulated PPP occurs in pathological conditions, particularly in Metabolic Syndrome, including hyperglycaemia (high blood glucose), the main dietary cause of which is high sugar (sucrose, fructose) consumption.
Excess dietary SUGAR → Metabolic Syndrome, Hyperglycaemia, Cardiometabolic Dysfunction → More PPP → More PPP Metabolites, such as Erythritol.
When there is a fire → firemen get into trucks → drive to the fire → there are multiple firemen at the fire. Do firemen cause fires?
Based on everything we understand about biology, biochemistry and years of scientific evidence, cardiometabolic dysfunction instigates higher PPP and higher erythritol, NOT the reverse. Why didn’t the authors acknowledge this? Let’s hope this was not scientific ignorance. If you’re going to publish a paper, please take 30min to read the existing scientific evidence about the topic first and carefully consider the implications for your paper.
Nature + Biology = Smart + Energy Efficient
Why is the PPP upregulated in cardiometabolic disease? The PPP plays a key role in antioxidant defence, recycling the body’s important antioxidant glutathione, in other antioxidant mechanisms and even in producing Nitric Oxide (key to helping blood vessels maintain healthy endothelial function). Could erythritol itself be contributing to the protective functions of the PPP? It has been demonstrated to have antioxidant properties and may protect endothelial function (the core blood vessel function that protects against atherosclerotic cardiovascular disease progression). Note that the last study on endothelial function was industry-funded. When in doubt, we should consider that usually, the body is doing its best to help us to survive and function. There is usually a ‘positive’ reason for it to be using energy to produce and do things.
Whether or not endogenous erythritol is actively protective, produced by the PPP ‘on purpose’ to help counteract the oxidative stress caused by the hyperglycaemic and cardiometabolic dysfunctional state as we might hypothesise, the key point is that it is a biomarker, a ‘signal’ of elevated PPP, and PPP is elevated in the diseased state. Is it surprising that those patients who had elevated levels of a key biomarker for disease (i.e. patients were more sick), had worse outcomes? If there are more firefighters at a fire, it’s probably because the fire is worse than another fire with fewer firefighters. Note: oddly, the authors did not in fact include the actual outcome data in this paper.
Part 2: Let’s Create Highly Pathological, Artificial Conditions to Get an Outcome
- A) The authors made platelet rich plasma (this is not blood in its ‘normal’ state, it is made to have a high concentration of platelets) from ‘healthy volunteers’ (who knows, the only criteria in the Methods says “no chronic disease” diagnosed), and mixed in “two known platelet agonists as follows: adenosine diphosphate (ADP) and thrombin receptor-activated peptide (TRAP6)”. These ‘agonists’ cause aggregation. They then added up to 270μg erythritol and noted an increased aggregation. In the washed platelets part of the experiment where they did NOT add in the aggregation factors ADP/TRAP6, NOTHING HAPPENED with up to 270μg erythritol.
- B) “Microfluidic shear flow experiments were performed using the Cellix Microfluidics System (Cellix) as previously described in refs. 51–53. Where indicated, each microchannel of a Vena8 Fluoro+ biochip was coated with type 1 collagen (15 µl; 50 µg ml−1). Images were collected using an HC Plan Apo 20X/0.7NA lens on a Leica DMI6000 inverted microscope equipped with an environmental chamber and a Hamamatsu ImagEM cooled CCD camera. Whole blood was incubated with an Alexa Fluor 488-conjugated antihuman CD42b antibody (303914, Biolegend; 5 μl/100 μl blood) and was pretreated with erythritol (45 μM) or normal saline (control) for 30 min at 22 °C…” In this biochip test, there appears on the photography to be more platelet adhesion with erythritol vs. saline (salt water), and 0 for both without collagen. One wonders what would happen with any other addition to this coated biochip…
- C) “Twelve- to 14-week-old BL/6J mice were injected with vehicle (normal saline), erythritol (25 mg kg−1) or 1,5-AHG (25 mg kg−1) and anesthetized with 100 mg kg−1 ketamine + 10 mg kg−1 xylazine. Rhodamine 6G (100 μl; 0.5 mg ml−1; 252433, Sigma) was injected into the right jugular vein to label platelets. The left carotid artery was then injured with a Whatman filter paper of 1 mm2 size containing 10% FeCl3 (157740, Sigma) for 1 min.” Instead of 13min for the saline vehicle and 14min for 1,5-AHG, it took 9min for the 290μg erythritol-injected mice’s injured carotid artery to cease bleeding through clotting. “The ferric chloride injury is now a well-established technique to rapidly and accurately induce the formation of thrombi in exposed veins or artery of small and large diameter.” So, they created a situation to INDUCE the formation of thrombi, and then noted a difference in minutes taken for the inevitable to happen. Again, one wonders what would happen with other injections. Vitamin K aids in blood clotting. Should we avoid consuming vitamin K containing foods? Should we aspire to bleeding to death when injured?
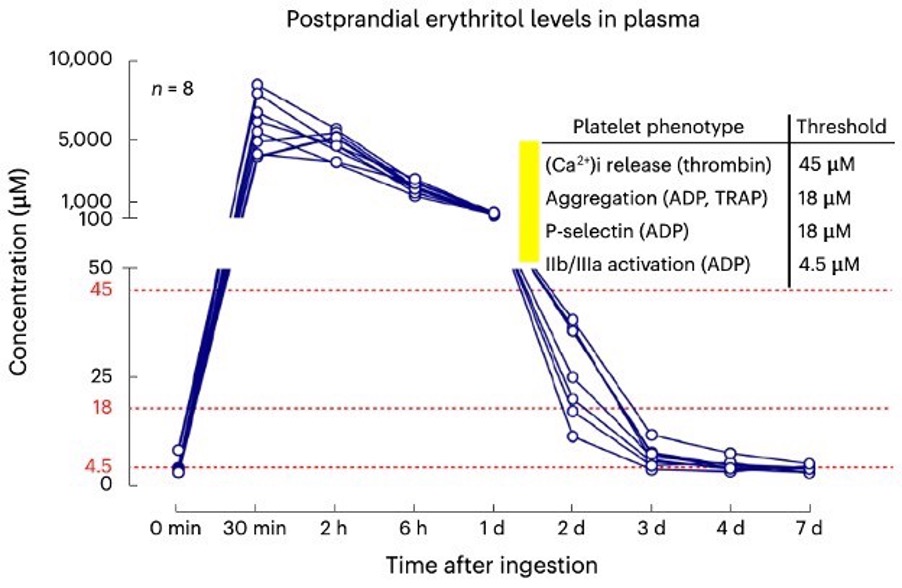
- D) Finally, they tested postprandial levels of erythritol after ingestion of 30g (a very high amount in 1 sitting and higher than what is permitted in beverages — max. 5–11g/330ml in the EU and US respectively), in LIQUID (faster absorption) form. They made 8 people ingest this liquid — not sure why it is 8, since the trial registration stated it would be c. 40 people. Did they test 40 people and then select (cherry pick?) 8 results, or simply decide to use only 8 people for some other reason? Who knows. Either way, plasma erythritol levels increased after the drink ingestion, returned to 100μg after 24hrs, and back down c. 5μg-40μg after 48hrs, flattening out at 4.5μg thereafter. They imply that these levels correlate with the levels they tested in their induced thrombotic platelets test conditions: ADP, TRAP, thrombin (see below highlight). Again, all of these artificial conditions INDUCE aggregation and thrombosis. Is anything useful being demonstrated here really?
End of the Study: When the answer is staring you in the face…
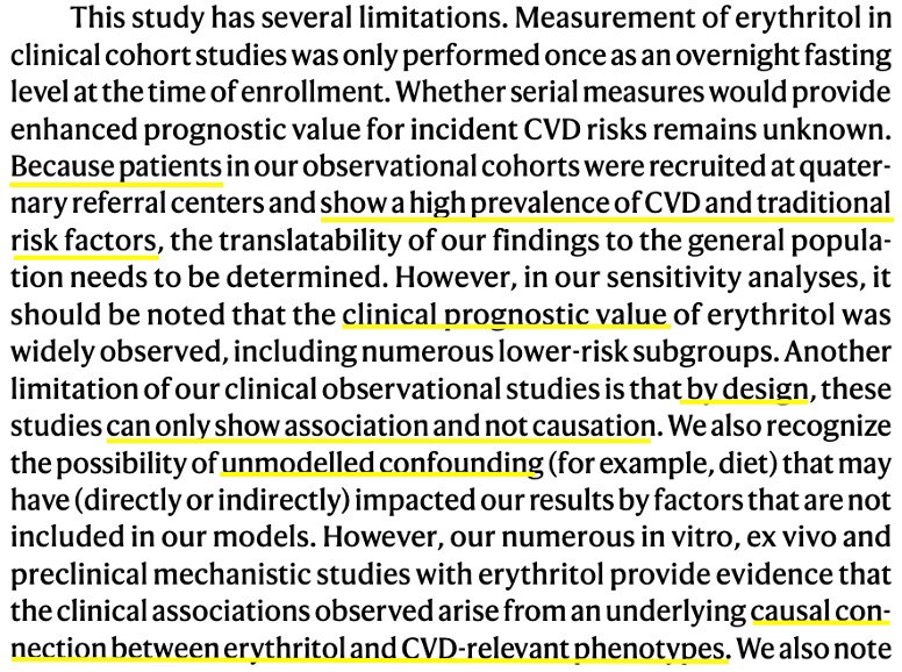
They accept these limitations and they almost seem to get it, but didn’t quite say it, or notice it (?!), the reverse causality of it all. CVD phenotype leads to → higher endogenous erythritol levels, not the opposite. This is not news either. We know already that in cardiometabolic dysfunction, the pentose phosphate pathway is elevated, including its metabolites, incl. erythritol — it is everywhere in the scientific literature. It indeed has “clinical progonostic value”. Have the authors not read about this? I sincerely hope that there is something unscrupulous going on, because if this was a true attempt at science, and if this was honestly peer reviewed by honest and educated scientists, I am very concerned about the future of science, truth-seeking, and frankly of the fate of humanity.
Conclusion
This was a very odd study on cohorts of people with severe cardiometabolic disease, with no randomisation, 6 primary outcomes, scarce background reading or context, highly artificial conditions for the in vitro and mouse testing, that, as with many poor studies, concluded what actually may be the polar OPPOSITE of truth. Why does this even matter and what is the very sad irony about this? This matters because people make dietary decisions based on headlines. Sadly, even well-known doctors who have evidently not read the study themselves immediately published it to their audience. This is bizarre to me — do they not care about their reputations when the truth eventually comes out as it usually does in the end? Do they not feel responsible to scrutinise the evidence first before pontificating?
What this fake news does is nudge people towards staying with the ‘devil they know’ — SUGAR — the very dietary culprit that in excess, directly, indisputably, causes the cardiometabolic dysfunction that this paper highlights. My MSc Dissertation was a Mechanism Review of Fructose and Atherosclerosis (CVD) — I spent years deep in this. SUGAR (sucrose, fructose) is a very real contributor and can be for many patients, THE LEADING INITIATORY CAUSE of metabolic syndrome and atherosclerotic cardiovascular disease. That is the very sad irony. Many people may develop metabolic syndrome and suffer chronic disease because of this paper that nudges them to stay with sugar and abandon truly viable ways to have healthy sweetness.